|
|
|
|
|
|
|
|
P Stewart,R Stewart
|
|
|
Ir Med J. 2012 Mar;105(3):83-4
P Stewart, R Stewart
Donegal Specialist Training Programme in General Practice, Education Centre, St Conals, Letterkenny, Co Donegal
Abstract
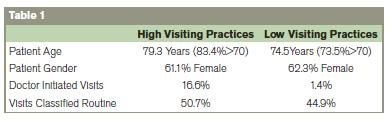
Data including information on patient age, gender, who initiated the visit and call classification was collected during office hours from 12 G.P. rural teaching practices with a combined GMS patient population of 24,720, over a 2 month period. There were a total of 603 home visits, giving an annual visiting rate of 143/1000. Visiting rates varied between practices from 45 to 305/1000 per year. When high visiting practices (>210/1000/year) were compared to low visiting rate practices (>90/1000/year), patients tended to be older (79.7 v 74.5 years) and calls were 12 times more likely to be doctor initiated (16.6% v 1.4%) or classified as routine( 50.7% v 44.9%). The variation between practices was related in part to patient age but appears largely due to differences in doctor home visiting behaviour. There are no recent figures on home visiting in Ireland.
|
Introduction
Several studies have reported wide variation in home visits, with rates varying from less than 1% in the United States to 10.1% of GP contacts in England and Wales1,2. A general decline in home visits has also been noted3-5. Studies have further observed a large variation in home visiting rates between practices2,9. Factors found to be associated with home visiting rates include; age, sex and social class6,7, with women, the elderly and the more socially deprived being more likely to seek domiciliary care8. The vast majority of home visits involves elderly patients (> 65 years) and are requested by either the patient or their carer6,9.
Methods
The aim of this study was to determine both the rate and factors associated with the variation in home visiting between Donegal G.P. training practices. Data was collected on home visits during office hours (08:00 – 18:00 Monday to Friday), from 12 teaching practices in the Donegal over a two month period in 2009. The study covered a total population of 24,720 GMS patients, all entitled to comprehensive free primary care and looked after by 29 GP principals and 12 registrars. Participating practices were given a standardized record sheet with strict definitions for each parameter measured. The data included information on patient age, gender and who requested the call (patient/relative, doctor, other). Calls were classified as either ‘Emergency’ requiring immediate response, ‘Urgent’ requiring a response within 24 hours or ‘Routine’ calls defined as calls which could wait until the following day.
Results
There were 603 calls in total during the two month study period. The mean home visiting rate was 143/1000/year. There was a 9 fold variation in rates between practices from 45 to 305/1000/year. When the three practices with the highest visiting rates (> 210/1000/year) were compared to findings for the three practices with the lowest visiting rates (< 90/1000/year),), patients tended to be older (79.7 v 74.5 years), female (62.3 v 61.1%) and calls were 12 times (16.6% v 1.4%) more likely to be doctor initiated or classified as ‘Routine’( 50.7% v 44.9%).
Discussion
Home visits are not only appreciated by patients but are also a valuable tool in primary care, allowing general practitioners to gain useful insights into a patient’s living conditions including their family and social supports. Home visits also provide an important service for the elderly and the house bound. Rates of home visiting have been declining and are known to vary considerably between different health care systems8. Australian rates for home visiting have decreased from 158/1000/year in 1997 to 77/1000 in 20074. Our mean home visiting rate of 143/1000/year compares favorably with these figures. Wide variations in visiting rates within health care systems have also been recorded2. Our study noted a 9 fold variation between practices which is much higher than reported elsewhere2. When comparing practices, both the patient age profile/gender and the calls classified as ‘Routine’, as expected, were higher in the high visiting practices. The most surprising finding in our study was that ‘doctor initiated calls’, varied by a factor of 12 between practices with high visiting rates when compared to practices with low home visiting rates. This variation appears to be largely due to differences in doctor home visiting behaviour.
The study was confined to a relatively small number of calls over a short time frame, within a rural setting and without taking into account seasonal variations or out of hour’s workload. Only GMS patients were included because of the lack of an accurate total practice population denominator in Irish general practice. A long overdue National survey of G.P. workload would help address these limitations as would qualitative research into the attitudes of family physicians towards home visits. Finally it remains to be seen whether the recent reduction in GMS funding (1st January 2011) and in particular the removal of patient domiciliary distance in calculating capitation payments, will adversely affect Irish home visiting rates in the future.
Acknowledgments
Trainers Workshop, Donegal Specialist Training Programme.
Correspondence: JPR Stewart
Donegal Specialist Training Programme in General Practice, Education Centre, St Conals, Letterkenny, Co. Donegal.
Email: [email protected]
References
1. Meyer GS, Gibbons RV. House calls to the elderly – a vanishing practice among physicians. NEJM 1997:18,337: 815-1820.
2. Aylin P, Majeed FA, Cook DG. Home visiting by general practitioners in England and Wales. BMJ 1996; 313: 207-210.
3. Nakar S, Vinker S, Weingarten MA. The place of home visiting in family practice: a multicentre comparison between rural and urban physicians .BJGP 1999; Vol. 49,445: 621-625.
4. Joyce C, Piterman L. Trends in GP home visits. Aust Fam Physician. 2008: 37(12):1039-42.Unwin B, Jerant A. The Home Visit, J. American Academy Family Practice 1999:60:1481-1488.
5. O Sullivan C, Omar RZ, Forrest CB, Majeed A. Adjusting for case mix and social class in examining variation in home visits between practices. Family Practice. 2004:Vol.21, No.4.
6. Bucquet D, Jarman B, White P. Factors associated with home visiting in an inner London general practice. BMJ (Clin Res Ed):290(6480):1480-1483.
7. Peppas G, Theocharis G, Karveli E, Falagas M. An analysis of patient house calls in the area of Attica, Greece BMC Health Serv Res 2006; 112.
8. Boerma WGW, Groenwegen. GP home visiting in 18 European countries adding the role of health system features. European Journal of GP 200:vol.7, No 4, 132-137.
9. Burton j, Leff B. The future of Home Care and Physician House Calls in the United States. The Journal of Gerontology 56: M603-M608:2001.
|
|
|
|
Author's Correspondence
|
|
No Author Comments
|
|
|
Acknowledgement
|
|
No Acknowledgement
|
|
|
Other References
|
|
No Other References
|
|
|
|
|