|
|
|
|
|
|
|
|
F O'Kelly,KT Lim,B Hayes,William Shields,N Ravi,JV Reynolds
|
|
|
Ir Med J. 2012 Mar;105(3):86-7
F O'Kelly, KT Lim, B Hayes, W Shields, N Ravi, JV Reynolds
Department of Clinical Surgery, St James’s Hospital, James’s St, Dublin 8
Abstract
We present a unique case of perforative appendicitis that occurred in an adult following blunt abdominal trauma. This case represents the first such reported case from Ireland. It also represents a modern practical example of Laplace’s theory of the effect of increased pressure on colonic wall tension leading to localized perforation, and serves to highlight not only the importance in preoperative imaging for blunt abdominal trauma, but also the importance of considering appendiceal perforation
|
Introduction
The magician and actor Harry Houdini died in hospital from peritonitis secondary to a ruptured vermiform appendix on Halloween 1926. He had sustained (permissive) abdominal trauma whilst performing1. There have been a small number of publications suggesting cases of blunt abdominal trauma causing appendicitis, the first of which was published in 19442, however even this is pre-dated by anecdotal reports as far back as 1892, a year before McBurney described his muscle-splitting incision. Ramsook outlining the proposed aetiology of traumatic appendicitis in childhood suggested four criteria that require to be fulfilled prior to association been proposed3. These consisted of an absence of prior abdominal complaints. The direct trauma should be severe and to the abdominal wall, the symptoms must commence 6-48hr afterwards and there must be surgical confirmation of appendicitis. The adult presented in this case, satisfied all the above.
Case Report
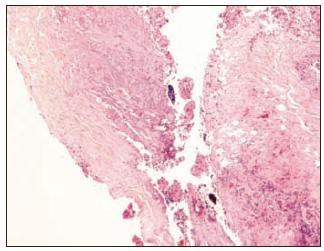
A 29-year old man presented to the A/E department of our institution with a 24-hour history of sudden, progressive right lower quadrant pain following a kick to the abdomen during a soccer game. The patient was resuscitated in accordance with ATLS® guidelines and demonstrated right iliac fossa guarding and rebound tenderness. There was no evidence of rigidity, and scrotal and digital rectal examinations were unremarkable. Biochemical markers displayed a leucocytosis (17.47x109/L) and a neutrophilia (13.2x109/L) with an increased serum lactate (2.7mM/L). Serum parameters were otherwise normal. A CT scan of the abdomen and pelvis showed evidence of an inflammatory lesion in the right iliac fossa with evidence of haemoperitoneum (Figure 1). The patient underwent a lower midline exploratory laparotomy which revealed a disintegrated perforated appendix. The stump was plicated, the peritoneal cavity irrigated, and the patient made an unremarkable post-operative recovery. Histopathology confirmed the presence of a disintegrated appendix specimen with evidence of a dense inflammatory infiltrate and necrotic fragments, correlating with a traumatic mechanism of injury (Figure 2).
Figure 1: CT study demonstrating inflammatory mass in the right iliac fossa with associated enlarged lymph nodes, free air, stranding and thickening of the adjacent caecum, small bowel and appendix

Figure 2: Histological specimen demonstrating the presence of inflammatory infiltrates within the appendiceal wall fragment
Discussion
The majority of reports have focused on paediatric cases presenting with recurrent abdominal pain. Houry et al. presented a case of abdominal trauma leading to diagnosis at laparotomy following radiographic studies demonstrating right colonic inflammation4. Etensel et al. retrospectively reviewed 29 cases of blunt paediatric abdominal trauma resulting in emergency presentations, of which five were found to have had appendicitis. This study highlighted the need to consider appendicitis in abdominal trauma and suggested a possible causal relationship, but that imaging modalities such as sonography and CT should be considered prior to operative management5. Derr et al. presented a case of an adult who was diagnosed with appendicitis following a right-sided water impact during cliff-diving and advocated the use of sonography in blunt abdominal trauma6.
As a result of the small number of publications of adult appendicitis following blunt abdominal trauma, there is no consensus regarding aetiology. We acknowledge that we cannot be certain that blunt abdominal trauma is merely co-incidental to an underlying diagnosis of appendicitis, although this is unlikely. Some reports including studies of seatbelt injuries following road traffic accidents have hypothesized that a sudden increase in abdominal pressure transmits pressure via increases in intraluminal bowel pressures to the caecal pole and appendix, especially in the presence of a competent ileocaecal valve. This in addition to external bowel wall compression can lead to seromuscular tears and perforation7. In cases of appendiceal injury, increases in luminal pressure may also impair blood circulation in the mesoappendix leading to an acute inflammatory response. This effect may be compounded if the appendix is compressed against the ilium. The vermiform appendix is also unusual in that it often contains faecoliths, which are twice as common in cases of traumatic appendicitis (60%-65%) compared to non-traumatic appendicitis, and may also be accountable in this condition’s aetiology8,9.
Correspondence: JV Reynolds
Department of Clinical Surgery, St James’s Hospital, James’s St, Dublin 8
Email: [email protected]
References
1. Houdini Historical Center. OCHS 1999 HoudiniHistorical Center Facts
2. Williams A.F: Traumatic perforation of appendix. British Medical Journal 1944, 1: 423
3. Ramsook C: Traumatic Appendicitis: Fact or Fiction? Paediatr Emerg Care 2001, 17: 264-266
4. Houry D, Colwell C, Ott C: Abdominal Pain in a Child after BluntAbdominal Trauma: An Unusual Injury. J Emerg Med 2001, 21: 239-241
5. Etensel B, Yazici M, Gursoy H,Ozkisacik S, Erkus M: The Effect ofblunt abdominal trauma on the Vermiform Appendix. Emerg Med J 2005, 22: 874-877
6. Derr C, Goldner DE: Posttraumatic Appendicitis: furtherextending the extended Focused Assessment with Sonography in Trauma examination.Am J Emerg Med 2009, 27: 632 e5-7
7. O’Kelly F, O’Brien GC, Broe PJ: Severe abdominalinjuries sustained in an adult wearing a pelvic seatbelt: a case report andreview of the literature. Ir J Med Sci 2008, 177: 385-387
8. Maes U, McFetridge E: Traumatic appendicitis. Am J Surg 1935, 30: 478-482
9. Arnbjornsson E, BengmarkS: Role of obstruction in thepathogenesis of acute appendicitis. AmJ Surg 1984, 147: 390-392
|
|
|
|
Author's Correspondence
|
|
No Author Comments
|
|
|
Acknowledgement
|
|
No Acknowledgement
|
|
|
Other References
|
|
No Other References
|
|
|
|
|