N Mc Grath, P Fitzpatrick, I Okafor, S Ryan, O Hensey, AJ Nicholson
Children’s University Hospital, Temple St, Dublin 1
Abstract
The use of adult seat belts without booster seats in young children may lead to severe abdominal, lumbar or cervical spine and head and neck injuries. We describe four characteristic cases of lap belt injuries presenting to a tertiary children’s hospital over the past year in addition to a review of the current literature. These four cases of spinal cord injury, resulting in significant long-term morbidity in the two survivors and death in one child, arose as a result of lap belt injury. These complex injuries are caused by rapid deceleration characteristic of high impact crashes, resulting in sudden flexion of the upper body around the fixed lap belt, and consequent compression of the abdominal viscera between the lap belt and spine. This report highlights the dangers of using lap belts only without shoulder straps. Age-appropriate child restraint in cars will prevent these injuries
Introduction
Motor vehicle crashes are the leading cause of death and acquired disability for children older than one1. Child fatalities and injuries in motor vehicles have been significantly reduced since the initiation of occupant protection measures in the 1970’s. Appropriate child safety seats are recommended for pre-school children and booster seats and later booster cushions are recommended until the child fits properly in the vehicle seat belt (usually 9 to 10 years of age).2 Lap Belt Syndrome (LBS) refers to serious cervical and lumbar spinal cord injuries in association with intra-abdominal injuries resulting from ill-fitting lap and shoulder belts1-3. The clinical triad for lap belt injury includes abdominal wall bruising, signs of spinal cord injury and hollow viscous organ injury. Standard lap belts are designed to restrain an adult just below the centre of gravity at the pelvis.1 However the immature anatomy of a child’s pelvis cannot provide anchor points for the belt until the child is at least 10 years old as in children the lap belt lies across the lower or mid abdomen rather than at pelvis level.2 Furthermore the lap belt may ride further up the abdomen if the child sits in a slouched position3. Sudden deceleration causes the spine to flex at the upper lumbar level rather than at the hips which may result in severe injuries of the abdomen and of the lumbar spine.
Small bowel perforation is the most common of the hollow viscous injuries. The diagnosis of bowel perforation is frequently delayed. Many perforations are initially subtle and come to the attention of physicians with increasing abdominal tenderness over time. An abdominal wall contusion significantly increased the likelihood of an intra-abdominal injury. There are two main types of lumbar spine injuries, compression fractures and Chance fractures. Chance fractures are hyperflexion injuries in which there is distraction of the posterior elements and impaction of the anterior components of the spine. Up to 50% of individuals with Chance fractures may also have serious blunt injury to internal organs.
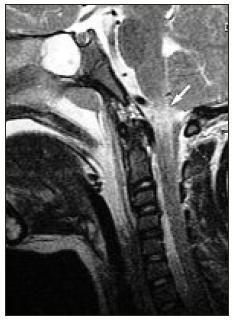
Figure 1: 6 year old boy. T2 sagittal MRI shows injury at junction of medulla and cervical cord (arrow).
Case Reports
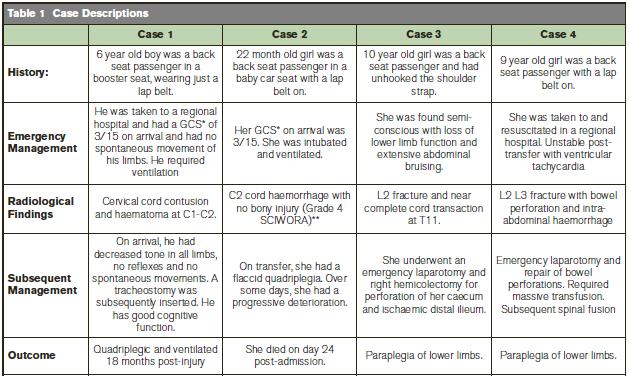
The case reports are summarized in Table 1. Their ages ranged from 22 months to 10 years (mean 8.5 years). All four children were rear seat passengers in significant motor vehicle accidents. All four were restrained by lap belts only. Two patients had cervical cord injury without spinal fractures and two had thoracic cord injury with lumbar spinal fractures and bowel perforation (see Figures 1 and 2). One child died 24 days post-injury, and one child is quadriplegic and requires mechanical ventilation 24 months later. Both children with lower cord injury remain paraplegic.
Figure 2: 9-year-old girl. (a) Sag CT reconstruction shows fracture separation of superior aspect of L3 vertebra. (b) Sagittal reconstruction more laterally shows complete dislocation of facet joints at L2/3 level. (c) 3D reconstruction of the CT shows fracture of superior aspect of L3 and dislocation of the facet joints at L2/3 level.

* GCS = Glasgow coma scale ** SCIWORA = Spinal cord injury without radiological abnormality
Discussion
Few population-based studies have been conducted that provide a reliable estimate of the prevalence of lap belt injuries among child occupants in car crashes. In general terms, our case series mirrors international experience. In 1987, Agran et al4 published one of the first population- based studies of paediatric restraint related injuries. A total of 1642 children injured as occupants in motor vehicle crashes were identified using an emergency department based surveillance system .Among this group, 191 (12%) were reported to be wearing a seat belt at the time of the crash. Three belted children (1.5%) were identified with intra abdominal injuries related to the seat belt. A total of ten children (5%) were described as having a seat belt- related abdominal wall contusion. In the largest case series of 98 children with LBS treated at the Children’s National Medical Centre in Washington DC between 1991 and 1997, the mean age of patients was 7.3 (+/- 2.5) years and over 70% were between 5 and 9 years6.
A very high proportion of 5 to 9 year olds use an adult seat belt for restraint instead of a booster seat or cushion. Often even when shoulder straps are available these are not used because they tend to ride up onto the face of a small child. A crash surveillance system based on a representative sample of children in 1999 showed a significant proportion of children between 2 and 5 years to be restrained in seat belts.7 Despite high restraint usage however, more than one third of children in this age range were inappropriately restrained by vehicle seat belts. This inappropriate restraint use resulted in a 3.5 fold increased risk of significant injury and more than a fourfold increased risk of significant head injury. In this study, among the 5311 children between 2 and 5 years restrained by seat belts, 11 (0.2%) were reported to have intra-abdominal or spinal injuries while no child in this group restrained with either a child safety seat or booster seat suffered an intra-abdominal injury. In 2006, Zurynski et al10 reported 20 cases of lap belt syndrome where over 85% were restrained with an adult lap belt without a booster seat. 13 were admitted to intensive care and 11 required surgery. There was one fatality and one child remained paraplegic. A similar surveillance study in Canada11 documented severe lumbar spine fractures and spinal cord injuries in children restrained by lap-only belts with 25% of LBS cases remaining paraplegic.
Children should be restrained in cars by means of a three-point anchor and this is only achieved by means of using a shoulder strap in addition to a lap belt. We support the accepted international view that they should remain in booster seats until they are the appropriate height and weight for seat belts7-9. This case series illustrates clearly that we need to increase professional and parental awareness on proper restraint use in child car passengers10,11.
Correspondence: AJ Nicholson
Children’s University Hospital, Temple St, Dublin 1
Email: [email protected]
References
1. Kelleher BJ, Walsh MJ, Dance DM, Gardner WT. An experimental study of the effects of child restraint improper installation and crash protection for larger size children. Warrendale, PA: Society of Automotive Engineers, 1983.
2. Johnson DL, Falci S. The diagnosis and treatment of pediatric lumbar spine injuries caused by rear seat lap belts. Neurosurgery 1990; 26: 434-441.
3. Glassman SD, Johnson JR, Holt RT. Seatbelt injuries in children. J Trauma 1992; 33: 882-886.
4. Agran P , Dunkle D , Wimn D. Injuries to a sample of seatbelted children evaluated and treated in a hospital emergency room . J Trauma 1987; 27: 58-64
5. Talton DS, Craig MH, Hauser CJ, Poole GV. Major gastroenteric injuries from blunt trauma. Ann Surg 1995; 61: 69-73
6. Huelke DF, Mackay GM , Morris A. Vertebral column injuries and lap-shoulder belts. J Trauma 1995; 38: 547-556.
7. Flaura K. Winston, Dennis R. Durbin, Michael J. Kallan, and Elisa K. Moll. The danger of premature graduation to seat belts for young children. Pediatrics 2000; 105: 1179-1183
8. American Academy of Paediatrics. Selecting and using the most appropriate car safety seats for growing children: Guidelines for counseling parents. Available at http://www.aap.org/family/01352htm
9. Durbin DR, Arbogast KB, Moll E. Seat belt syndrome in children: A case report and review of the literature. Pediatric Emergency Care 2001; 17: 474-477
10. Katie N Reeve, Yvonne A Zurynski, Elizabeth J Elliott, Lynne Bilston. Seatbelts and the law: how do we protect Australian children? Medical Journal of Australia 2007; 186: 635-638
11. Cyr C, Lemoine C, Santschi M. Canadian Paediatric Surveillance Program 2005 results. Canadian Paediatric Society, Ottawa, 2006, 28-9.