|
|
|
|
|
|
|
|
J Cryan,Niamh Ó Catháin,M Curtis,M Cassidy,FM Brett
|
|
|
|
Ir Med J. 2010 Nov-Dec;103(10):303-5.
|
|
J Cryan1, N Ó Catháin1, M Curtis2, M Cassidy2, FM Brett1
1Department of Neuropathology, Beaumont Hospital, Beaumont, Dublin 9
2State Pathologist’s Office, Malahide Rd, Marino, Dublin 3
Abstract
Excessive drinking increases the risk of dying unnaturally. In the Republic of Ireland such deaths are referred to the State Pathologist. Blood alcohol concentration (BAC) is routinely measured. We created a database of cases presenting to the State Pathologist over a nine year period (2000-2008 inclusive) to evaluate the relationship between alcohol and fatal traumatic brain injuries (FTBI). Of a total of 1778 cases, 332 (275 Male [M]; 57 Female [F]) died of head injuries. Fatalities were highest in males aged 36-50 (N=97) and 26-35 (N=73). Assaults (N=147), falls (N=95), road traffic accidents (RTA) (N=50) and suicide (N=15) were the commonest modes of presentation. A positive blood alcohol concentration (BAC) was found in 36% of assaults, 41% of falls and 40% of suicides. In the RTA group BAC was positive in 59% of pedestrians, 33% of drivers and 14% of passengers. Alcohol clearly plays a significant role in FTBI in the forensic setting.
Introduction
The association between alcohol consumption and violence relates to acute intoxication. In a culture where drinking often leads to intoxication one would anticipate an increase in violence. Thus a strong association between alcohol sales and violent behaviour was found in Sweden where ‘explosive’ drinking is not unusual compared with France, where drinking occurs in the context of dining1. In the last decade, alcohol consumption has increased in Ireland with Irish drinkers currently among the highest consumers of alcohol in Europe2. A study in 2002 comparing Ireland’s drinking habits, with six other European countries (known as ECAS countries - Finland, Sweden, Germany, Britain, France and Italy) showed that drinking occasions in Ireland more often involves ‘binge drinking’ compared with other European countries3. Adverse consequences related to single drinking occasions are not uncommon in Ireland3. In a previous study we showed that the contribution of alcohol to FTBI in the acute hospital situation was underestimated largely because alcohol was not routinely checked in the Emergency Department (ED)4. The aim of this study was to ascertain the role of alcohol in FTBI’s in the Forensic service where BAC is routinely performed.
Methods
The autopsy records from 2000 up to and including 2008 (N=1778) in the State Department of Forensic Medicine were reviewed for cases coded as “traumatic brain injury”. A database was then created using Microsoft Access. The gender, age, interval from presentation to death, mechanism of injury, cause of death and blood alcohol concentration (BAC) were all recorded. Interval from presentation to death was specifically examined to ascertain any delay between the incident and subsequent death. Where there was a delay, the BAC at autopsy would be irrelevant whereas the BAC at presentation would be important and BAC was sought from the hospital records. The cause of injury (whether assault, RTA, suicide, fall or unknown) was recorded. The method used - blunt force, gun shot, stab wounds - was documented for assaults and suicide. If the patient was dead on arrival in the ED, the BAC was obtained from the autopsy records. BAC in Ireland is measured in milligrammes of alcohol per millilitre of blood. A concentration of 1 gramme of alcohol per 1 millilitre of blood indicates a BAC of 100%. As alcohol is known to impair judgment at levels lower than the legal limit, the presence of any alcohol in the blood samples was considered a “positive” case5.
Figure 1: Age at autopsy
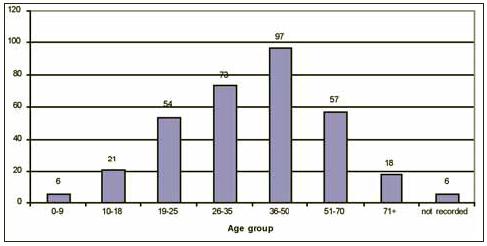
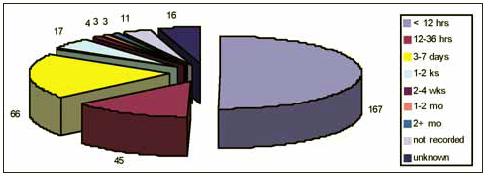
Figure 2: Interval before autopsy
Results
332 cases (275M; 57F) fulfilled the criteria for inclusion. Fatalities were highest in males aged 36-50 years (N=97) and 26-35 (N=73) (Figure 1). The interval between the incident and autopsy was less than 12 hours in 50% of cases (Figure 2). The positive BAC samples ranged from <100 to > 500 mg %. Assaults (147) (128M; 19F) were the commonest mechanism of injury followed by falls, RTA’s and suicide (Figure 3). The majority of assaults occurred in males in the age group 26-35. A positive BAC was found in 54/147 (36.7 %) of cases (M50; F4). BAC in the remaining 93 cases was negative in 52/147 (35.34%) and the remainder were not checked as there was either a delay before autopsy or the remains were unsuitable. Blunt force (N=60) (48 M; 12 F) head injury was the commonest mechanism of assault, followed by gun shot wounds (N= 40) (38 M; 2F).
Figure 3: Mechanism of injury
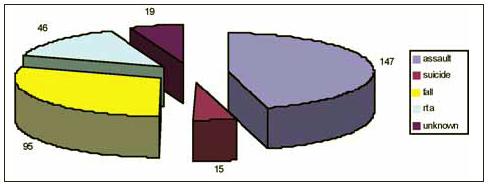
Figure 4: Death due to falls

Falls (95) (M 72; F23) were the second commonest cause of TBI. The majority of falls occurred in males in the age group 36-50 (Figure 4). A positive BAC was found in 38/95 (40%) (M30: F8). In 37/95 (38%) it was unrecorded and the remaining 20 were negative. RTA’s accounted for 50 cases (pedestrians (N=39, passengers (N=7) and drivers (N=4)). A positive BAC was found in 23/39 pedestrians (58.9%) (M 22: F1). In 9 cases (23%) it was not recorded and in 7 (17%) BAC was zero. Of the 4 drivers, a positive BAC was found in 2/4 (50%) (M 2). Suicide (N=15) (M15) was the last major category. A positive BAC was found in a 6/15 (40%) of suicides examined. Gun shot (N=13) was the commonest method used.
Discussion
The contribution of alcohol to FTBI is underestimated in the acute hospital setting4. This has consequences whether the patient survives or dies6. Inaccurate or incomplete certification of the cause of death in alcohol related diseases is not uncommon6,7. Alcohol-related illness, death or injury is one of the greatest public health issues in Ireland currently5. In this study, 50% of cases came to autopsy less than 12 hours after the incident and as BAC testing is done as a routine, the true contribution of alcohol to unnatural FTBI deaths can be assessed.
Alcohol plays a role in violent behaviour but many people drink often and to excess without violent consequences. Its role varies according to the cultural context and social situation involved8. Generally both perpetrators and victims are male and the severity of the violence relates to the volume and type of alcohol consumed9. In this study, we are dealing only with victims and the majority are male. A positive BAC was found in 36% of assaults who died of FTBI. The age (26-35) and gender (M) is similar to that in Scotland10. Here blunt force was the commonest method used, supporting observations from other studies that victims of FTBI are usually males killed by acquaintances, during a fight11. The object used reflects what is immediately available. Guns are the commonest method used in the USA. They are also popular in Australia, Canada and Italy12. English, Welsh and Scottish offenders rarely use firearms but tend to favour, as in this study, blunt force13. Assaults with guns are more likely to end in death compared with other weapons12. In other words, guns have a high lethality index or ‘completion’ rate14.
Falls were the second commonest cause of FTBI and occurred in a younger age group (36-50) than FTBI in the acute hospital setting4. A positive BAC was found in 40% in keeping with previous observations that alcohol-related falls are associated with an increased incidence of head injuries and increased severity of the resultant injury15. With respect to RTAs, most of our cases were male. This is similar to other studies, suggesting that males are more likely to be involved in RTAs, whether driver, passenger or pedestrian16. Pedestrians (58.9%) in this study, and in other studies, had the highest BAC compared with drivers and passengers16,17. Intoxicated pedestrians are more likely to suffer severe trauma to the head, thorax and abdomen than their sober counterparts18. This is clearly significant with respect to liability and insurance claims.
Suicide victims were all males, peaking in the middle age (36-50). Older suicides differ from those occurring in a younger age group, as they are less likely to have attempted suicide previously or have a ‘documented’ psychiatric history and are more likely to be ‘successful’19. This ‘success’ reflects the lethal methods used. Here, guns were the commonest method accounting for 86% of cases. A positive BAC was found in 40% which is higher than studies carried out by Medical Examiners in the US where rates varied between 30 and 38% of cases20,21. It is thought that ethanol may undermine the weakly constructed barrier against suicide that can be relied upon by the suicidal personality in sobriety. This study clearly demonstrates that alcohol plays a significant role in FTBI in the forensic setting. Continued media coverage of the harmful effects of binge drinking together with lack of acceptance of it as the ‘norm’ may eventually make it unpalatable. Public awareness groups have proved successful in this venture in the USA22.
Correspondence: J Cryan
Department of Neuropathology, Beaumont Hospital, Beaumont, Dublin 9
Email: [email protected]
References
1. Rossow I. Alcohol and homicide: a cross-cultural comparison of the relationship in 14 European countries. Addiction, 2001 Feb;96 Suppl 1:S77-92.
2. Strategic Task Force on Alcohol. Interim Report.. Department of Health and Children, 2002.
3. Ramstedt M, Hope A. The Irish drinking habits of 2002- Drinking and drinking-related harm in a European comparative perspective. J. Substance Use, 2005; 10 (5): 273-283.
4. O'Toole O, Mahon C, Lynch K, Brett FM. Is the contribution of alcohol to fatal traumatic brain injuries being underestimated in the acute hospital setting? Ir Med J. 2009 Jul-Aug;102:207-9.
5. Bellis M, Bolster M, Doyle C. The role of alcohol in deaths presenting to the coroner's services in Cork City and County. Ir Med J. 2009 Jan;102:13-5
6. Maudsley G, Williams EM. "Inaccuracy' in death certification--where are we now? J Public Health Med, 1996; 18: 59-66.
7. Maxwell JD, Knapman P. Effect of coroners' rules on death certification for alcoholic liver disease. Br Med J (Clin Res Ed). 1985 Sep 14;291:708
8. Pridemore WA. Vodka and violence: alcohol consumption and homicide rates in Russia. Am J Public Health. 2002 Dec;92:1921-30
9. Klatsky AL, Armstrong MA. Alcohol use, other traits, and risk of unnatural death: a prospective study. Alcohol Clin Exp Res. 1993 Dec;17:1156-62
10. Leylad AH, Dundas R. The social patterning of deaths due to assault in Scotland, 1980-2005: a population -based study. J Epidemiol Community Health. 2010 May;64:432-9
11. Lo M, Vuletic JC, Koelmeyer TD. Homicides in Auckland, New Zealand. A 14-year study. Am J Forensic Med Pathol. 1992 Mar;13:44-9
12. Abel EL. Guns and blood alcohol levels among homicide victims. Drug Alcohol Depend. 1986 Nov;18:253-7.
13. Gillies H. Homicide in the West of Scotland. Br J Psychiatry, 1976 Feb; 128: 105-27.
14. Beaman V et al. Lethality of firearm-related injuries in the United States population. Ann Emerg Med. 2000 Mar;35:258-66
15. Johnston JJ, McGovern SJ. Alcohol related falls: an interesting pattern of injuries. Emerg Med J. 2004 Mar;21:185-8
16. Elliott S, Woolacott H, BR. The prevalence of drugs and alcohol found in road traffic fatalities: a comparative study of victims. Sci Justice. 2009 Mar;49:19-23.
17. Hain JR, Ryan DM, Spitz WU. Fatal accidents and blood ethanol levels in adolescents and adults. The Wayne County experience, 1978-1988. Am J Forensic Med Pathol. 1989 Sep;10:187-92
18. Mittmeyer HJ. Severity of injury of alcohol intoxicated pedestrians in street traffic. Beitr Gerichtl Med. 1991;49:247-51
19. Sher L. Alcohol consumption and suicide. QJM. 2006 Jan;99:57-61.
20. Mendelson WB, Rich CL. Sedatives and suicide: the San Diego study. Acta Psychiatr Scand. 1993 Nov;88:337-41
21. Shields LB, Hunsaker DM, Hunsaker JC 3rd, Ward MK. Toxicologic findings in suicide: a 10-year retrospective review of Kentucky medical examiner cases. Am J Forensic Med Pathol. 2006 Jun;27:106-12
22. Fell JC, Voas RB. Mothers against drunk driving (MADD): the first 25 years. Traffic Inj Prev. 2006 Sep;7:195-212.
|
|
|
|
Author's Correspondence
|
|
No Author Comments
|
|
|
Acknowledgement
|
|
No Acknowledgement
|
|
|
Other References
|
|
No Other References
|
|
|
|
|