Introduction
Breast cancer is the most commonly diagnosed cancer worldwide and the second leading cause of female cancer deaths.1 A deleterious mutation in the BRCA2 gene has been associated with breast cancer rates of 45%.2 Pregnancy-associated breast cancer (PABC) is defined as breast cancer occurring during pregnancy, lactation or the first postpartum year. PABC is seen in less than 1/3,000 pregnancies,3 yet accounts for 10-20% of breast cancers in women under 30. Incidence is increasing as more women delay child-bearing.4 As the majority of PABCs occur in women less than 40, BRCA mutations are more common in this patient group.5
Case Report
A 30-year old woman, at 35 weeks gestation, was referred by her General Practitioner to our breast clinic with a 2-week history of a right breast lump. Her family history was significant in that her 49-year old mother had recently been diagnosed with breast cancer and been found to carry a pathogenic BRCA2 mutation. Clinical examination revealed a palpable lump in the right breast. Protected mammography demonstrated pleomorphic calcifications spanning 3.8cm. Ultrasonography revealed a 2.8cm area of hypoechogenicity corresponding to the area of clinical and mammographic concern (Figure 1). Core biopsy was performed. Analysis of biopsied tissue revealed grade 2 invasive lobular carcinoma (ILC).
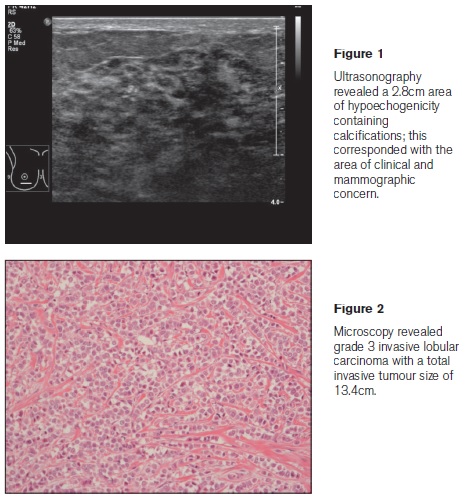
Urgent predictive genetic testing was performed at the patient’s request and she was found to carry the familial BRCA2 mutation. Following multidisciplinary case discussion, labour was induced at 38 weeks. Delivery was uncomplicated. Following further case review and counselling, the patient underwent upfront sentinel lymph node biopsy. When this proved positive for metastatic disease, she went on to have a right mastectomy with tissue expander reconstruction and axillary clearance. Histopathological analysis of resected tissue revealed grade 3 ILC extending over 13.4cm, oestrogen receptor positive, human epidermal growth factor receptor 2 negative (Figure 2). Margins were clear. Four of 36 lymph nodes were positive for metastatic disease. Postpartum, the patient was referred to the Human Assisted Reproduction Ireland unit with a view to oocyte freezing prior to initiation of adjuvant chemotherapy. Further treatment will include radiotherapy and hormonal therapy. The patient will continue to have close surgical follow-up with 6-monthly alternate mammograms/ Magnetic Resonance Imaging (MRI) scans. A prophylactic left mastectomy will be considered at some time in the future. She will also have 6-monthly CA125 levels and pelvic ultrasounds with a view to bilateral prophylactic salpingo-oophorectomy.
Discussion
Patients with PABC should be managed as non-pregnant patients, with some modifications to protect the foetus.6 In this case, as the patient was 35 weeks pregnant at the time of diagnosis, pregnancy could be expedited and treatment initiated postpartum, without risk of adverse maternal or foetal outcome. This case was further complicated by the discovery of a BRCA2 mutation during pregnancy. Management options for BRCA mutation carriers with breast cancer include: Ipsilateral mastectomy for management of the known breast cancer and bilateral mastectomy with prophylaxis on the contralateral side, given the increased risk of both ipsilateral and contralateral breast cancers.7 In this case, given that the patient had T3N2a breast cancer, it was decided that the known cancer be dealt with first and that prophylactic mastectomy be delayed.8 In high risk patients in whom prophylactic surgery is deferred, close surveillance with regular clinical breast examinations, annual mammography and breast MRI is indicated.8 Tamoxifen may lower the risk of contralateral breast cancer in BRCA carriers with a history of breast cancer.9 Pregnancy during or after a diagnosis of breast cancer does not adversely affect survival in BRCA mutation carriers.10 This case highlights the difficulties associated with management of BRCA-associated breast cancer, particularly in the setting of pregnancy. Optimal management necessitates multidisciplinary involvement.
Correspondence: C Ní Leidhin
St Vincent’s University Hospital, Elm Park, Dublin 4
Email: [email protected]
Acknowledgements
Departments of General, Breast and Endocrine Surgery, Pathology and Radiology, St. Vincent’s University Hospital, Elm Park, Dublin 4
References
1. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. GLOBOCAN 2008 v1.2, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 10 [Internet]. Lyon, France: International Agency for Research on Cancer, 2010.
2. Antoniou A, Pharoah PD, Narod S, Risch HA, Eyfjord JE, Hopper JL, Loman N, Olsson H, Johannsson O,Borg A, Pasini B, Radice P, Manoukian S, Eccles DM, Tang N, Olah E, Anton-Culver H, Warner E, Lubinski J, Gronwald J, Gorski B, Tulinius H, Thorlacius S, Eerola H, Nevanlinna H, Syrjäkoski K, Kallioniemi OP,Thompson D, Evans C, Peto J, Lalloo F, Evans DG, Easton DF. Average risks of breast and ovarian cancer associated with BRCA1 or BRCA2 mutations detected in case Series unselected for family history: a combined analysis of 22 studies. Am J Hum Genet. 2003 May;72:1117-30.
3. Eedarapalli P, Jain S. Breast cancer in pregnancy. J Obstet Gynaecol. 2006 Jan;26:1-4.
4. Anders CK, Johnson R, Litton J, Phillips M, Bleyer A. Breast cancer before age 40 years. Semin Oncol. 2009 Jun;36:237-49.
5. Shen T, Vortmeyer AO, Zhuang Z, Tavassoli FA. High frequency of allelic loss of BRCA2 gene in pregnancy-associated breast carcinoma. J Natl Cancer Inst. 1999 Oct 6;91:1686-7.
6. Amant F, Loibl S, Neven P, Van Calsteren K. Breast cancer in pregnancy. Lancet. 2012 Feb 11;379:570-9.
7. Hartmann LC, Schaid DJ, Woods JE, Crotty TP, Myers JL, Arnold PG, Petty PM, Sellers TA, Johnson JL, McDonnell SK, Frost MH, Jenkins RB. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N Engl J Med. 1999 Jan 14;340:77-84.
8. Saslow D, Boetes C, Burke W, Harms S, Leach MO, Lehman CD, Morris E, Pisano E, Schnall M, Sener S,Smith RA, Warner E, Yaffe M, Andrews KS, Russell CA; American Cancer Society Breast Cancer Advisory Group. American Cancer Society guidelines for breast screening with MRI as an adjunct to mammography. CA Cancer J Clin. 2007 Mar-Apr;57:75-89.
9. Phillips KA, Milne RL, Rookus MA, Daly MB, Antoniou AC, Peock S, Frost D, Easton DF, Ellis S, Friedlander ML, Buys SS, Andrieu N, Noguès C, Stoppa-Lyonnet D, Bonadona V, Pujol P, McLachlan SA, John EM, Hooning MJ, Seynaeve C, Tollenaar RA, Goldgar DE, Terry MB, Caldes T, Weideman PC, Andrulis IL, Singer CF, Birch K, Simard J, Southey MC, Olsson HL, Jakubowska A, Olah E, Gerdes AM, Foretova L, Hopper JL. Tamoxifen and risk of contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. J Clin Oncol. 2013 Sept 1;31:3091-9.
10. Valentini A, Lubinski J, Byrski T, Ghadirian P, Moller P, Lynch HT, Ainsworth P, Neuhausen SL, Weitzel J,Singer CF, Olopade OI, Saal H, Lyonnet DS, Foulkes WD, Kim-Sing C, Manoukian S, Zakalik D, Armel S,Senter L, Eng C, Grunfeld E, Chiarelli AM, Poll A, Sun P, Narod SA; Hereditary Breast Cancer Clinical Study Group. The impact of pregnancy on breast cancer survival in women who carry aBRCA1 or BRCA2 mutation. Breast Cancer Res Treat. 2013 Nov;142:177-85.