|
|
|
|
|
|
|
|
Nuala Healy,Hong Kuan Kok,Catherine Wall,W Torreggiani
|
|
|
Sir
We read with great interest the excellent and informative case report by Tevlin et al describing a case of Erdheim-Chester disease (ECD), a form of non Langerhans cell histiocytosis, of the gastrointestinal tract.1 In the case presented by the authors, a laporotomy was required for definitive diagnosis, as percutaneous biopsy of the retroperitoneal adenopathy was non diagnostic. We would like to share a similar case of this rare disorder, encountered recently in our institution, where a different approach was utilized by performing a percutaneous renal biopsy allowing for the correct diagnosis to be made without the need for laporotomy.
|
|
A 63 year old male presented with recurrent episodes of exertional chest pain and dyspnoea. He had a background of stage 3 chronic kidney disease, renal artery stenosis, hypertension and previous ischaemic stroke. A CT thorax on admission revealed bilateral pleural effusions with pleural enhancement and overlying subsegmental atelectasis with scattered foci of consolidation. A cuff of soft tissue was noted around the entire thoracic and abdominal aorta, consistent with a periarortic infiltrative process. Concentric, non-enhancing soft tissue masses were also seen to encase and involve both kidneys, particularly the left with somewhat reduced perfusion of the left renal parenchyma (Figure 1). Bilateral renal artery stents were present from previous percutaneous intervention for renal artery stenosis. Right pleural drainage was performed and biochemistry confirmed an exudative efffusion. Ultrasound guided biopsy of the left kidney and perinephric soft tissue was also performed, the histology of which revealed fibroconnective tissue with sclerosis, scattered chronic inflammation, and admixed macrophages (CD68 positive, S100 negative). No mutation in the BRAF gene was identified, which has been reported in 50% of ECD. The case was discussed at the Haematology multidisciplinary meeting. Based on the histological findings of the left renal and perinephric soft tissue biopsy, periaortic infiltration and resultant renal artery stenosis, a diagnosis of ECD was made. Isotope bone scan did not reveal any osseous features associated with ECD, however bone involvement although common, is not a diagnostic requirement. Our patients acute presenting symptoms resolved following drainage of the pleural effusions. He was commenced on interferon-alpha therapy and remains well at follow-up.
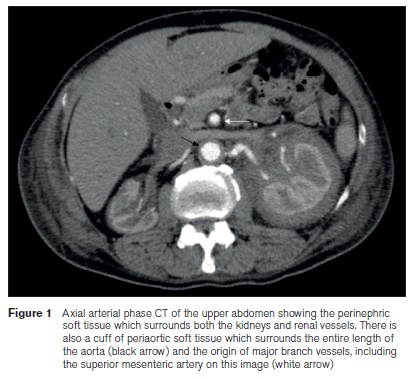
Diagnosis of ECD can prove challenging as alluded to in the case report by Tevin et al, due to the variable presentation, ranging from asymptomatic subtle soft tissue infiltration to involvement of multiple organs.1 The imaging findings described above in our case were typical and highly suggestive of the diagnosis from the outset, but biopsy was ultimately required for confirmation. It was fortunate that the perinephric soft tissue mass was amenable to percutaneous image guided biopsy and surgery was not required to confirm the diagnosis. Indeed, Figure 1 from the case by Tevin et al, demonstrates a cuff of periaortic soft tissue which was similar to our case. In contrast, our patient did not display involvement of the gastrointestinal tract. Although rare, ECD should be considered when an infiltrating retroperitoneal process is encountered on imaging studies as patients may be asymptomatic in the initial stages.
NA Healy, HK Kok, C Wall, W Torreggiani
Department of Radiology, AMNCH, Tallaght, Dublin 24
References
1. Tevlin R, Cahalane AM, Larkin JO,Treacy A, Connaghan D, Winter DC. Gastrointestinal Erdheim-Chester disease. IrMed J 2014; 107.
|
|
|
|
Author's Correspondence
|
|
No Author Comments
|
|
|
Acknowledgement
|
|
No Acknowledgement
|
|
|
Other References
|
|
No Other References
|
|
|
|
|