Introduction
Personal firearms are strictly licensed in Ireland and can only be owned under strict conditions. This has been suggested as a reason for the low rates of firearm injuries traditionally seen in Ireland. Redmond HP et al published a review of ten years of gunshot injuries in 19851 and found 21 injuries, 20 of which were with low velocity weapons, and four of whom died. Recent increased use of handguns in Ireland heralded a marked increase in mortality, to 8 of 17 (47%) in a paper published in 20082, whereas mortality from low velocity (shotgun) injuries was 1 / 31 (3%). Information from Northern Ireland during the years of conflict there showed that low velocity weapons were used for “punishment” by paramilitary organizations3, which after the ceasefire of August 1994 was largely replaced by punishment beatings4. Appropriate imaging plays a crucial role in evaluation and management of firearm injury, especially high velocity (e.g. handgun) injury. Computed tomography (CT) can identify the site of the bullet and elucidate surrounding organ damage, to a far greater extent than radiography. Interventional radiology is increasingly required for management as well as diagnosis. Magnetic resonance imaging (MRI) has a limited role to play as the projectiles are metallic.
Methods
All patients presenting or brought by ambulance to Connolly Hospital Emergency Department (ED) between 2001 and 2010 were eligible for inclusion. A prospective database had been maintained of patients presenting with gunshot injuries. A chart review was carried out. Patient demographics and imaging performed for each patient were reviewed.
Results
65 patients with gunshot injuries were seen in the emergency department between 2001 and 2010, of whom charts were available in 59. The patients were aged between 15 and 52 (mean age 27.4), and only one was female. 29 gave their profession as unemployed, and 10 were from the travelling community in Ireland. As previously demonstrated, mortality for high velocity wounds was much higher (10/23, 43%) than for low-velocity shotgun injuries (2/34, 6%). It was also shown that bullet wounds tended to be focused around the torso, head and neck, and shotgun wounds tended to be concentrated around the peripheries. 8 patients died in the ED. Of the 51 patients that survived beyond the ED, 43 had radiography, and 15 had CT scans in the emergency setting, and a further 10 had follow up CT scans. 5 patients were transferred for emergent management in interventional radiology. Four patients underwent emergency ultrasound scans.
Discussion
The results show a dramatic increase in gun crime in Dublin over the previous 4 decades. The age profile had decreased (mean age 27 years, decreased from 31), and the mortality had increased, with a marked increase in high-velocity firearms, i.e. handguns, rifles and semi-automatic weapons. This has been widely attributed to increased gangland activity and the illegal drug trade. In a study published in 2005 in the European Journal of Public Health, mortality from opioid misuse had increased 15-fold from 1980 to 1999 in Ireland5. The number of firearm related injuries is still quite low by comparison with other developed nations. Cook County Hospital in Chicago in 1995 showed 476 gunshot wounds over a ten year period6; Prince Mshyeni Memorial Hospital, Durban, South Africa examined 78 gunshot injuries in just 6 months7. In both countries, gun ownership is less stringently controlled than in the Republic of Ireland.
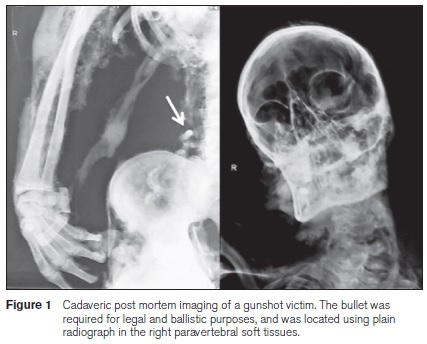
The experience gained in large urban centres can be useful in dealing with gunshot injury, as it relatively rare in Irish residency training8. Despite the fact that some patients had succumbed to their injuries prior to medical assistance, many are still referred to the radiology department. During the period of the study, 15 cases underwent post-mortem radiological scanning. These cases are usually for forensic and legal purposes e.g. for dental age estimation9, or bullet retrieval (see Figure 1). Conclusion: There has been a sharp increase in the numbers of admissions from gunshot injuries in a West Dublin hospital in the Republic of Ireland in the past decade. Despite this, the numbers in Ireland are still low by comparison with other developed countries, and the burden on our radiology department remains relatively low. Should the increasing trend continue, further resources and expertise may be required.
Correspondence: IG Murphy
St Vincent's University Hospital, Elm Park, Dublin 4
Email: [email protected]
References
1. Redmond HP, Lane BE. Ir J Med Sci. A 10 year review of gunshot injuries in a Dublin teaching hospital. 1985; 154: 395-6.
2. Murphy IG, Kneafsey B. Gunshot injury in west Dublin over a 5-year period: a plastic surgery perspective. J Plast Reconstr Aesthet Surg. 2008; 61: 1240-1
3. Nicholas RM, Barr RJ, Mollan RA. Paramilitary punishment in Northern Ireland: a macabre irony. J Trauma. 1993; 34: 90-5.
4. Eames MH, Kneafsey B, Gordon D. A fractured peace: a changing pattern of violence. Br J Plast Surg. 1997; 50: 416-20.
5. Kelleher MJ, Keown PJ, O'Gara C, Keaney F, Farrell M, Strang J. Dying for heroin: the increasing opioid-related mortality in the Republic of Ireland, 1980-1999. Eur J Public Health. 2005; 15: 589-92.
6. Stone JL, Lichtor T, Fitzgerald LF, Barrett JA, Reyes HM. Demographics of civilian cranial gunshot wounds: devastation related to escalating semiautomatic usage. J Trauma. 1995; 38: 851-4.
7. Chamisa I. Civilian abdominal gunshot wounds in Durban, South Africa: a prospective study of 78 cases. Ann R Coll Surg Engl. 2008; 90: 581-6.
8. McWeeney DM Walker TW Gilbert FJ McCarthy PA. Radiology trainees in the UK and Ireland: academic background, publication rates and research plans. Br J Radiol. 2009; 82: 1033.
9. Kvaal SI, Kolltveit KM, Thomsen IO, Solheim T. Age estimation of adults from dental radiographs. Forensic Sci Int. 1995; 74: 175-85.
