A O'Farrell1, D De La Harpe1, U Geary2
1Health Intelligence Unit, HSE, Stewarts Hospital, Palmerstown, Dublin 20
2Department of Emergency Medicine, Emergency Directorate, St James’s Hospital, Dublin 8
Abstract
The aim of this study was to describe the epidemiology and impact of serious assault warranting in-patient care over six years and its impact on ED attendances in a large teaching hospital in Dublin over 2 years. There were 16,079 emergency assault-related in-patient hospital discharges reducing from 60.1 per 100,000 population in 2005 to 50.6 per 100,000 population in 2010. The median length of stay was 1 day (1-466) representing 49,870 bed days. The majority were young males (13,921, 86.6%; median age 26 years). Overall crime figures showed a similar reduction. However, knife crimes did not reduce over this period. Data on ED attendances confirmed the age and gender profile and also showed an increase at weekends. Alcohol misuse was recorded in 2,292/16079 (14%) of in-patient cases and 242/2484 (10%) in ED attendances. An inter-sectoral preventative approach specifically targeting knife crime is required to reduce this burden on health services.
Introduction
There is a common perception in the media that the rate of violent crime and in particular assaults involving knives are on the increase.1,2 However, Irish crime figures show that the number of reported serious assault offences categorised as “Assault causing harm” have decreased in recent years. Figures for the period 2005-2010 show that the number of reported offences categorised as “Assault causing harm” have been on a downward trajectory with the number decreasing since the highest number recorded in 2006.3 However, there is evidence to show that more than 50% of assaults presenting to hospital are not reported to the police4 and it has been suggested that data from health providers may contribute to a more accurate assessment of the burden serious assault has on society.5 Furthermore, there is in-sufficient data on the effect of cases of serious assault on acute hospital workloads. The aim of this study was to describe the epidemiology and impact of serious assault (i.e. assault serious enough to warrant hospital in-patient care) on acute hospitals; to determine if the incidence of hospital in-patient admissions for assault due to the use of knives has increased over time. Further aims were to describe the impact of assault on ED attendances in a large teaching hospital in Ireland and compare these figures to the number of reported serious assault offences over the same study period.
Methods
This study involved the use of two datasets. The first dataset was the Hospital In-patient enquiry (HIPE) database and the second was the Emergency Department (ED) database from a large teaching hospital in Dublin. Patients admitted as an emergency to all acute hospitals in the Hospital In-Patient Enquiry (HIPE) database with any diagnosis of assault (ICD Code 10 X85-Y09) were identified and extracted for years 2005-2010. HIPE is a computer-based health information system that collects data on discharges from acute public hospitals in Ireland.6 The HIPE database contains information on the patient’s age, sex, area of residence, date of admission and discharge, together with their principal diagnosis and up to 20 other diagnoses, coded using the International Classification of Diseases, Tenth Revision (ICD10).7 To calculate assault-related hospital in-patient rates, the number of hospital in-patient discharges was used as numerator and the total resident population as the denominator. The total resident population data were extracted from the Health Atlas database that includes census and inter-censual data from the Central Statistics Office of Ireland.8 Rates were standardized to the EU standard population (direct method).
Data were analysed using JMP statistical package.9 Crude and age-adjusted rates and rate differences were calculated using StatsDirect.10 T-tests were used to compare means. The Wilcoxon test was used to compare medians. The Pearson’s X2 test was used to compare proportions in groups of categorical data and test for trend was used to identify linear trend and regression slopes were compared using Stata.11 Emergency department (ED) attendance data for two years (i.e. 2009 and 2010) from one large teaching hospital in Dublin (2009-2010) was obtained. Ethical approval for the use of the ED data was obtained from the research ethics committee of the hospital.
Results
In-patient hospital discharges and number of reported assault offences:
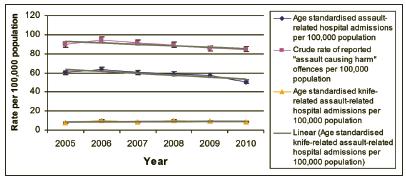
There were 16,079 assault-related hospital in-patient episodes i.e. assault related admissions that were severe enough to warrant in-patient hospital care over the 6 year study period (2005-2010). This total number is 6,850 less than the number of reported “Assaults causing harm offences” for the same study period (Table 1). The age standardised assault-related hospital in-patient discharge rate decreased significantly from 60.1 per 100,000 population in 2005 to 50.6 per 100,000 population in 2010 (Figure 1). The rate for reported “assault causing harm” offences per 100,000 population also reduced similarly over the study time period (Figure 1). However, the age-standardised rate for “assault with sharp object including knife” in-patient discharges did not decrease and remained stable over the study period (Figure 1).
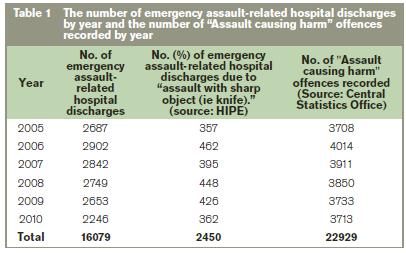
Figure 1: Assualt-related hospital in-patient discharges and "assault causing harm" related recorded offences per 100,000 population
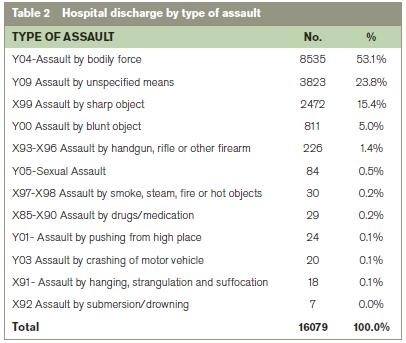
The most common principal diagnosis was head injury (10,070, 62.6%) followed by injuries to the wrist and forearm (1299, 8.1%) and injuries to the abdomen, lower back and pelvis (841, 5.2%). The majority of the patients were recorded as being admitted from home 15,312 (95.2%) and the most common mode of admission was via the ED (14,038, 87.3%). Median LOS was 1 days (Range =1-466). Total bed days used was 49,870 including 3,128 bed days in the Intensive Care Unit (ICU) averaging 8,313 bed days per annum. Those assaulted by a sharp object were 3.5 times more likely to need Intensive Care Unit (ITU) care (OR 3.49, 95% CI 2.96-4.93 p<0.001). Those assaulted by a sharp object were also 1.2 times more likely to die in hospital although this was not statistically significant (OR 1.21, 95% CI 0.66-2.20, p=0.54). The majority of the patients were discharged home (13,748, 85.5%) and 73 (0.45%) died in hospital. The majority of those who died in hospital (46, 63.0%) had “injuries to the head” followed by “injuries to the abdomen, lower back, spine and pelvis” (7, 9.6%) recorded as their principal diagnosis. The three most common types of assault among those who died were “assault by unspecified means” (24, 33.0%), “assault by blunt force” (22, 30.1%), “assault by sharp object including knife” (13, 17.8%) and assault by handgun or other firearms (6, 8.2%)
The most common types of assault were assault by bodily force (8535, 53.1%), assault by a sharp object including knives (2,472, 15.4%) and assault by a blunt object (811, 5%). The use of a firearm or gun as a method of assault was recorded in 2,256 (1.4%) of the cases (Table 2) with no significant increase over the six year study period. The majority of admissions (9,665, 69.9%) occurred at weekends. Alcohol and/or drug use was recorded for 2,292/16079 (14%) of the discharges.
Demographic profile
The majority of patients were male (13,921, 86.6%) and under 30 years old (8,453, 61.1%). The median age for males was significantly younger than the females (26 years vs. 28 year, p<0.001). The age and gender profile of patients did not change significantly over the 6 year study period. Patients recorded with an “Assault by sharp object” were significantly more likely to be male (92.6% vs. 7.4%) whereas “Assault by strangulation” (53% vs. 47%) was more common among the females.
Emergency Department (ED) attendances:
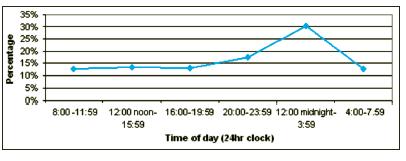
There were 2,484 ED attendances for assault to this Dublin teaching hospital during the period 2009-2010. In 2009, 1,175 (2.6%) of the 45,838 ED attendances were for assault and in 2010, 1,309 (2.9%) of the 45,230 ED attendances were for assault. Half of the ED assault attendances arrived by ambulance (1,242/2484, 50.0%) the remainder arrived either by walking in or by car, taxi, bus or by garda car. The majority were male (2,015, 81.1%) and the median age was 29 years (range 15-93 years) with no significant difference over the two year study period. The majority of the attendances were classified as urgent (1,385, 55.8%) or very urgent (252, 10.1%). The most common days for attendance were weekends and the most common time of attendance was between midnight and 4.00 a.m. (Figure 2). Data on type of assault were very poorly recorded in the ED database. A total of 1,861 (74.9%) had a head or facial injury recorded and 694 (27.9%) had an open wound/laceration recorded. Alcohol/drug misuse was recorded in 242 (9.7%) of the attendance records.
Figure 2: Assault related ED attendance by time of day
Discussion
This study has shown that the rate of serious assault (i.e., assault that requires in-patient hospital admission) per 100,000 population has been decreasing during the six year study period of 2005-2010. This corresponds to the decreasing trend in the rate of reported “assault causing harm offences” per 100,000 population observed over the same time period. It is interesting to note the number and rate of “assault causing harm offences” are higher year on year than the figures for in-patient hospital discharges with an assault-related diagnosis. However, some of these recorded offences may have resulted in ED attendances that did not warrant in-patient care, or injuries may have been dealt with by primary care services, or medical care may not have been sought. Our study also found that of the ED attendances at just one large Dublin teaching hospital during a study period of two years (2009-2010), a total of 2,484/91058 (2.7%) of attendances were due to assault. This study found those with an assault–related hospital in-patient admission and ED attendance were predominantly young males. Although alcohol and or drug use was recorded in some cases the quality of such recording appears variable and there is a clear need to improve its recording in assault-related admissions and ED attendances. The higher incidence at weekends reflects the increased prevalence of anti-social behaviour at weekends.
The lack of a reduction in knife crime together with the greater need for ICU care and the higher in-hospital mortality rate among those victims of knife crime are a great cause for concern and indicate that there is an urgent need to tackle knife crime among young Irish males. Evidence from international studies indicates that interventions that adopt a public heath approach (for example reducing risk factors such as alcohol and drug use) rather than a criminal justice approach have greater impact on reducing violence in a society.12 Thus public health professionals need to take a leadership role in ensuring that national policies for preventing violence among the young are developed and involve other stakeholders such as the local authorities and the justice system. Furthermore, the challenges posed by collecting ED-based data for this study highlights the need for standardised datasets to capture assault-related injury in EDs. The development of a national injury registry would greatly facilitate this endeavour.
Correspondence: A O'Farrell
Health Intelligence Unit, HSE, Red Brick Building, Stewarts Hospital, Palmerstown, Dublin 20
Email: [email protected]
References
1. Riegel R, Soaring rates of city knife crime prompts call for amnesty. http://www.independent.ie/national-news/soaring-rates-of-city-knife-crime-prompts-call-for-amnesty-3105748.html, in Irish Independent. 2012: Dublin. p. Sunday May 13th 2012.
2. Riegel R, Alarming rise in knife crime. http://www.independent.ie/national-news/alarming-rise-in-knife-crime-3126470.html, in Irish Independent. 2012: Dublin. p. Sunday June 3rd 2012.
3. Central Statistics Office, Recorded crime offences by type of offence 2004-2011. 2012.
4. Sutherland I, Sivarajasingam V, and Shepherd JP, Recording of community violence by medical and police services. Injury Prevention, 2002. 8: 246-247.
5. Maxwell R, Trotter C, Verne J, Brown P, Gunnell D. Trends in admissions to hospital involving an assault using a knife or other sharp instrument, England, 1997–2005. Journal of Public Health, 2007. 29: 186-190.
6. Department of Health and Children, Activity in Acute Public Hospitals In Ireland. 2012, The Economic and Social Research Institute.: Dublin.
7. International Statistical Classification of Diseases and Related Health Problems, World Health Organisation, in 10th revision. 1992: Geneva.
8. Central Statistics Office, Vital Statistics 2000-2010. 2010, CSO: Dublin.
9. SAS Institute, JMP statistical package. 2001: Cary NC, USA.
10. StatsDirect, StatsDirect statistical programme. 2003: Cheshire UK.
11. SAS Institute, Stata statistical package. 2002: Cary NC, USA.
12. Sethi D, et al., European report on preventing violence and knife crime among young people, World Health Organisation, Editor. 2010.: Geneva: viii + 102.
