Ir Med J. 2006 Jun;99(6):167-9
Abstract
This prospective observational study was undertaken to assess the impact of a major music festival on the workload of a local hospital. Data were collected on all attendances at Naas General Hospital from the nearby Oxegen 2004 music festival. Patient demographics, disposition and diagnoses were recorded. Emergency department activity levels were compared before, during and after the festival. Seventy-two attendees were referred to Naas emergency department over a 3-day period, representing a 45% increase in the hospital’s emergency department attendance rate. Thirty-seven of these attendees (51%) required inpatient or tertiary centre services. Thirty-four attendees (47%) were noted as having consumed alcohol and /or used illicit substances. We conclude that despite the provision of on-site medical facilities, major music events are associated with a significant increase in local health care activity and expenditure.
Introduction
The impact of a music event on acute hospital services is significant with up to a 50% increase in local emergency department (ED) workload.1 Literature from the 1970s suggests that 1 of 75 patrons attending large outdoor music concerts can be expected to need medical attention.2 More recent literature puts the figure seeking medical aid at approximately 1 per 1000 patrons.3,4 There is also variability in the literature regarding the number of attendees at music events referred to the local hospital, 3,5- 9depending on the health care system and medical facilities on-site at the event.
The Oxegen 2004 music festival took place on July 10th & 11th at the Punchestown Racecourse, which is situated almost 5 kilometres from Naas in Co. Kildare. Approximately 80,000 people attended this outdoor event. This figure includes the estimated 60,000 people who camped at Punchestown for the duration of the festival and the estimated 20,000 people who bought single day concert tickets each day. The campsite opened at 18.00hrs on July 9th and had closed by 17.00hrs on July 12th. It occupied the area within the 2-mile Punchestown racetrack. All medical referrals from Punchestown were brought to the local hospital, Naas
General Hospital (NGH). The aim of this study was to establish the impact of the Oxegen music festival on clinical activity at Naas General Hospital.
Methods
A three-tier medical care system as outlined by the “Code of Practice for Safety at Outdoor Pop Concerts and other musical events”10 was in operation on site at the Oxegen concert stadium in Punchestown. The medical care system consisted of 20 first aid teams, seven first aid posts and one medical centre. Two of the first aid posts provided 24-hour medical cover from 1800hrs on July 9th to 1200hrs on July 12th and were situated 3 kilometres from the concert stadium at the campsite. Due to its large size, the campsite was divided into campsites A and B and each had its own first aid post. All first aid teams consisted of 2 trained first-aid personnel. The staff at each first aid post included an emergency medical technician (EMT), a nurse with ACLS certification and a general practitioner. Physician staffing in the medical centre consisted of 6 doctors, one of whom had some formal anaesthetic training. This team included 5 non-consultant hospital doctors (NCHDs - registrars in anaesthesia or emergency medicine (EM) and EM senior house officers) with one EM consultant. These 6 physicians aided by 2 EM nurses staffed the medical centre between 1200hrs and 0200hrs on July 10/11th and between 1200hrs and 0100hrs on July 11/12th. Eight ambulances served the concert venue each night, six provided by the Eastern Regional Health Authority and two by the Order of Malta
A large marquee with floor space greater than 25 square metres was erected to create the on site medical centre. There were 2 resuscitation trolleys with monitoring equipment and anaesthetic trays. Also, there were twelve stretcher beds at floor level for observing and treating patients. Patient’s details were collected on 2-layer medical forms. One layer of this medical form accompanied any patient referred to the ED at Naas General Hospital. Of note, no patient was referred to NGH without adherence to the 3-tier system described and all referred patients had been assessed by doctors in the on site medical centre prior to their transfer.
The ED of Naas General hospital has one resuscitation room (two cubicles) and ten examination cubicles. It has 163 acute medical beds including four intensive care beds. The Adelaide & Meath Hospital (AMNCH - a tertiary referral centre) is a 20 minute ambulance ride from Naas General Hospital.
Any “Oxegen attendee” who registered with Naas ED between 00.01hrs on July 10th and 00.01hrs on July 13th, 2004 was prospectively identified. Patient details were collected on standard emergency department and inpatient case notes. Any medical forms accompanying the referred patients were also collected. Each patient was clinically assessed and blood alcohol levels and urine toxicology (Triage Tox-drug screen, Biosyn Diagnostics) were performed as clinically indicated.
Statistical analysis
Data are presented as median (range). Data were analysed using Stata Release 8.2. A regression model was used to estimate the normal weekend workload and its associated confidence interval and then to estimate the increase attributable to the festival with its confidence interval (CI).
Results
A total of 1355 festival goers (1.7% of the total number of attendees) sought medical attention between 18.00hrs on July 9th and 12.00hrs on July 12th, 2004. Of the 1355 attendees, 229 (0.3%) attended the first aid post at the Oxegen campsite and 1126 (1.4%) sought medical attention at the concert venue.
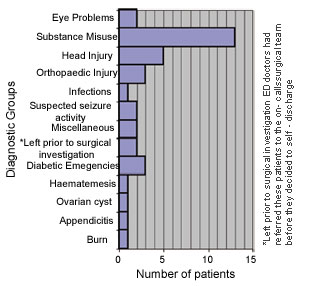
Of the 1355 attendees, 72 (5%) presented to Naas ED (Figure 1). Sixtyeight were referred by on-site medical personnel and transported to the ED by ambulance, 3 self-presented and a local general practitioner referred one. Forty-nine (68%) were male and 23 (32%) were female with a median age of 21 years (range 16-34 years).
 |
|
Figure 1 Number of festival attendees who
presented to the emergency department of Naas
General Hospital and their diagnostic groups |
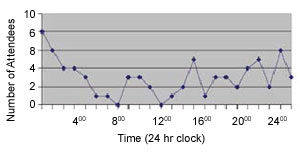
The time of arrival of the first Oxegen attendee was recorded as 00.28hrs on July 10th and the last as 17.28hrs on July 12th, 2004. Fourteen attendees (19.4%) registered with Naas ED between 01.00 - 03.00 hrs over the 3-day period, coinciding with the closure times of the on-site medical centre (Figure 2).
 |
|
Figure 2 Summative hourly
attendances at Naas emergency
department from 00.01 hours July
10th to 00.01 hours on July 13th. |
Hospital admissions and transfers
Of the 72 attendees who presented to Naas ED, 37 (51%) required inpatient or tertiary centre services of whom 31 were admitted to NGH (Figure 3) However, only 3 (4%) had an inpatient stay in NGH lasting more than 24 hours. Six patients were transferred to other hospitals. One patient had a burn surface area of 19% warranting transfer to the Burns Unit in St James Hospital, Dublin. Two patients had eye problems warranting transfer to the Eye and Ear Hospital, Dublin. A further 3 patients were transferred to the Orthopaedic Unit in the Adelaide & Meath Hospital, two with ankle fracture dislocations and one with multiple foot
fractures.
 |
|
Figure 3 Clinical conditions requiring
inpatient /tertiary management |
Alcohol and illicit substance use
Of the 72 attendees, 34 (47%) were noted as having consumed alcohol and /or used illicit substances. Twenty-four of the 72 festival attendees (33%) were noted to have consumed alcohol of whom 17 (24%) had recorded blood alcohol levels ranging between 191 – 431 mg/dl. Of the remaining seven festival goers in this subgroup: four did not have blood alcohol levels recorded and three recorded levels <21 mg/ dl but either tested positive for or admitted to using illicit substances.
Thirteen of the 72 attendees (18%) admitted to using illicit substances. Eight of this subgroup had a positive toxicology test: seven tested positive for ecstasy (of which 3 also tested positive for cannabis and/or cocaine) and one tested positive for cannabis alone. Of the remaining five festival attendees in this subgroup, four were not tested and one had a negative urine toxicology screen.
Of the 34 attendees who had consumed alcohol and/or used illicit substances, 23 (68%) were admitted to NGH from the ED: five had an associated head injury, two had reported seizure activity, one had haematemesis warranting upper GI endoscopy and two were transferred to the orthopaedic service in AMNCH. Thirteen of these admissions, representing 42% of the Oxegen-related admissions to NGH were related to substance misuse alone. Disposition of festival attendees not requiring hospital admission Of the 72 Oxegen attendees to Naas ED, thirty-five were not admitted to hospital. Eleven (15%) attendees were referred to outpatient departments and six (8%) were advised to attend their GP. Sixteen patients (22%) were treated and discharged to self-care and two patients (3%) did not wait to be seen. All 3 Oxegen attendees who self-referred to the ED were diagnosed with soft tissue injuries, discharged and one was advised to attend the ED review clinic.
Hospital workload
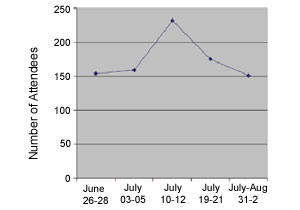
There was a mean ED attendance of 160 (95% CI 143 – 177) based on the surrounding weekends. Seventy-two extra attendances were recorded in the festival weekend, with an associated confidence interval of 34 to 100 (P = 0.009). The Oxegen festival weekend, therefore, saw a 45% increase in the hospital’s usual workload (Figure 4).
 |
|
Figure 4 Comparative weekend
emergency department attendances
before, during and after Oxegen
2004 |
Discussion
Music festivals significantly increase the workload of local hospital services. Although previous studies have documented the number of festival attendees referred to local hospitals for medical management, there is great variability in the literature.3, 5-9 The aim of this study was to establish the impact of a major music festival on the workload of our local hospital.
At Oxegen 2004, 1,355 attendees (1.7%) sought medical attention. This figure is comparable with recent literature from weekend festivals held in the UK and Ireland. At the1989 Cornwall weekend music festival (attendance 25,000), 1.9% of attendees sought medical attention.7 A 1970’s music festival lasting two and a half days with an attendance of 150,000 recorded a figure of 1.1% needing medical attention.8 Feile 1995 (also a 3-day festival but with an attendance of 70,000) recorded that 2.3% of attendees sought medical aid.5 These data support the suggestion that approximately 1 of 75 patrons (1.3%) attending large
outdoor music concerts will need medical attention2 rather than the figure of 1 in 1,000 patrons as quoted in more recent studies.3,4
Oxegen 2004 resulted in 72 extra ED attendances (CI 34 – 100) at NGH over a 3-day period. Thirty-one attendees (43%) needed admission with a further 6 attendees (8%) requiring transfer to another hospital. Our attendance data are also comparable with recent literature from similar sized events held in the UK and Ireland. The 3-day 1993 Glastonbury festival (attendance 85,000) resulted in 53 extra ED attendances and 24admissions to the nearby hospital (45% admission rate).11 Feile 1995 recorded a total of 92 “Feile related” ED attendances and 23 admissions to the 4 surrounding hospitals.5
The attending population was young, with a median age of 21 years and the majority of these patients were discharged within a 24-hour period. This is consistent with the age profile,6,11 and length of stay5 in previous studies. Minor trauma, substance misuse and head injury were common presenting complaints, as also demonstrated by previous studies.4 These studies report that diabetic emergencies and respiratory conditions, particularly among asthmatics, prompt attendees to seek medical assistance.6,11 Our study is no exception with 5 of the 72 attendees (7%) in this category.
Recent literature suggests that of those seeking medical aid at major rock concerts 48% admit to using illicit drugs or alcohol while on-site.4 This is comparable to the findings of the present study, which reports a rate of 47% (34 attendees) and is supported by blood alcohol levels and urine toxicology results. There is variability in recent Irish literature with Slane 1999 (1-day concert) reporting that 66% of attendees consumed alcohol.6 However, this figure was based solely on retrospective analysis of the patient details as recorded on the ED notes. Feile 1995 reports that 47.8% of admissions associated with the festival were related to alcohol and/or illicit substance use.5 Similarly, the present study records that 42% of the Oxegen-related admissions to NGH were due to substance misuse
alone.
This study demonstrates that despite the provision of on-site medical facilities, music festivals result in a significant increase in ED attendances at the local hospital, which in turn carries a sizeable financial burden. The“Code of practice for safety at outdoor pop concerts and other outdoor musical events”10 currently requires formal liaison with local health authorities at the “preliminary planning stage” of these events. It does not require that the medical directorate of the local ED be informed or involved in this planning process. In 1986, Sanders et al. published guidelines for medical care at mass gatherings stating “…in order to provide advanced life support services at events, appropriate arrangements must be made with paramedic provider agencies and base station hospitals.”12 Results
from our study support this suggestion.
References
- Murphy D, Jabbar N, Eldin M, Gillen P. Audit of the impact of a major pop concert on the workload of two regional hospitals. Irish medical
Journal, 2001; 94: 15
- Whipkey RR, Paris PM, Stewart RD. Emergency care for mass gatherings. Postgraduate Medicine 1984; 76: 44-7.
- De Lorenzo RA, Gray BC, Bennett PC, Lamparella VJ. Effect of crowd size on patient volume at a large, multipurpose, indoor stadium. Journal of Emergency Medicine 1989; 7: 378-384.
- Erickson TM, Aks SE, Koenigsberg M, Bunney EB, Schurgin B,Levy P. Drug use patterns at major rock concert events. Annals of Emergency Medicine 1996; 28: 22-26.
- Reddy S, Munro P, Luke CL, Cusack S. Feile ’95: Combining hospital and field care at a major music festival. The Irish Colleges of Physicians and Surgeons, 1997; 26: 107-110.
- Ryan JM, Noone E, Plunkett PK. Review of a mobile accident and emergency unit at a rock concert. Irish Medical Journal 1994; 87: 148-149.
- Chambers J, Guly H. The impact of a music festival on local health services. Health Trends, 1991; 23: 122-123.
- Schlicht J, Mitcheson M, Henry M. Medical aspects of large outdoor festivals. Lancet 1972: 948-952.
- Hewitt S, Jarrett L, Winter B. Emergency medicine at a large rock festival. J Accid Emerg Med 1996; 13: 26-27
- Irish Government Publications. Code of Practice for Safety at Outdoor Pop Concerts and other outdoor musical events 1996; Chapter 16: 63-68.
- Britten S, Whiteley MS, Fox PF, Goodwin MI, Horrocks MJ. The Glastonbury Festival 1993: pattern of attendances and admissions to an NHS Trust. J Accid Emerg Med 1995; 12: 30-31
- Sanders AB, Criss E, Steckl P, Meiskin HW, Raife J, Allen D. An analysis of medical care at mass gatherings. Ann Emerg Med 1986; 15: 515-519.